Based Directly on a Genuine BBC article ..

The term PCR test is understood by the majority of the public to be a well established, reliable and accurate way of determining whether someone does or does not have COVID-19 disease. This is the line strongly promoted by most governments and the MSM. That is far from the case and as the saying goes "it's more complicated than that "- in this case much, much more complicated.
The Wikipedia definition of PCR is :
Polymerase chain reaction (PCR) is a method widely used to rapidly make millions to billions of copies (complete copies or partial copies) of a specific DNA sample, allowing scientists to take a very small sample of DNA and amplify it (or a part of it) to a large enough amount to study in detail. PCR was invented in 1983 by the American biochemist Kary Mullis at Cetus Corporation. It is fundamental to many of the procedures used in genetic testing and research, including analysis of ancient samples of DNA and identification of infectious agents. Using PCR, copies of very small amounts of DNA sequences are exponentially amplified in a series of cycles of temperature changes. PCR is now a common and often indispensable technique used in medical laboratory research for a broad variety of applications including biomedical research and criminal forensics.[1][2]
A COVID-19 PCR test is based on the PCR process and essentially amplifies by repeated cycles the DNA/RNA from e.g a sample nasal swab. If target SARS- CoV2 viral RNA is detectable at or below a chosen number of cycles designated the Cycle threshold (Ct) the test is positive and the person providing the sample is deemed to have COVID-19 and if not detected by the designated Ct the test is negative and the person is deemed not to have COVID-19.
If your understanding of PCR tests is as described at the start of post alas your understanding is unfortunately almost entirely wrong. Consider these extracts from official and mainstream sources (not some random ill informed site on the web):
"RT-PCR detects presence of viral genetic material in a sample but is not able to distinguish whether infectious virus is present."
A single Ct value [i.e one PCR test] in the absence of clinical context [i.e The subject being tested has not been assessed by a clinician] cannot be relied upon for decision making about a person’s infectivity. n.b. the inserted text in [ ] are my clarifications
It’s also unclear to what extent people with no symptoms transmit SARS-CoV-2. The only test for live virus is viral culture. PCR and lateral flow tests do not distinguish live virus. No test of infection or infectiousness is currently available for routine use.678 As things stand, a person who tests positive with any kind of test may or may not have an active infection with live virus, and may or may not be infectious.9
“PCR detection of viruses is helpful so long as its accuracy can be understood: it offers the capacity to detect RNA in minute quantities, but whether that RNA represents infectious virus may not be clear.”
"The exact relationship (between Ct value and infectivity) is still being researched, and interpreting these results depends on the clinical context.
So picking apart the widely held understanding of mass of PCR tests for COVID 19 as outlined above:
"Polymerase chain reaction (PCR) tests are lab-based and test for the presence of SARS-CoV-2 virus."
"Daily and cumulative numbers of cases
Number of people with a positive COVID-19 virus test (either lab-reported or rapid lateral flow test) on or up to the specimen date or reporting date (depending on availability)."

It's now September 2021, some 18 months after the start of the "pandemic" (see below), and over 15 months since my last post. I had hoped something approaching normality would have returned by now along with an understanding of the SARS CoV2 virus, the associated disease COVID-19 and how best to treat /contain it from a medical and public health policy perspective. Alas that is not the case and while many aspects of the virus and associated disease are now relatively well understood many remain contentious e.g. the extent of asymptomatic spread, the level of transmission by touch, the effectiveness of social distancing and so called "lockdowns", the effectiveness of vaccines in preventing the spread of COVID-19, concerns over vaccine side effects and many more. Since my first post many of the polices adopted in early 2020 to try and deal with COVID-19 e.g. masks, restrictions on travel, work at home orders, forced isolation etc remain in place to some extent while others, compulsory testing, forced vaccination (for some), quarantines for travellers have been introduced.
What is however clear is that governments, many scientists and medical professionals and the majority of the mainstream media have not provided the public with clear, accurate and balanced information on the situation. The mainstream media have largely acted as both an uncritical and supportive mouthpiece for the prevailing government narrative and as click-bait alarmists providing endless highly emotive stories of individual suffering, ever rising death tolls", "spikes" "surging", highly deadly variants of the virus etc etc .
I consider that it is self evident that Governments and their uncritical supporters remain firmly in the grip of "groupthink" whereby they are so convinced of their own "rightness" they refuse to consider, and in many cases try to suppress and discredit, anyone and anything that questions or challenges the position they hold and policies they are implementing. A key element of groupthink is an "end justifies the means" mentality whereby those stuck in groupthink believe that any negative consequence of their actions however terrible are both morally and practically justified i.e. a price worth paying.
My aim remains to try and provide a more accurate and balanced view of what has happened over the last 18 months by analysing the main elements of the mainstream position and in some cases the counter narratives e.g. it’s all a fake "scamdemic". To start however it is essential to try and characterise the true extent of COVID-19 crisis - a term I will use as, whatever the true causes, there has been and remains a crisis - to help assess to what extent the polices imposed to deal with it were and remain justified.
If asked last last year what I considered a pandemic I would have said something like the medieval black death or the Spanish flu of the early 1900s that killed 10's of millions of otherwise healthy people world-wide. This understanding would probably be held by many others. A typical dictionary definition:
Definition of pandemic (Entry 1 of 2)
: occurring over a wide geographic area (such as multiple countries or continents) and typically affecting a significant proportion of the population
with an examples of usage being;
"The 1918 flu was pandemic and claimed millions of lives".
The definition of a flu pandemic used by the WHO until 2009 was: .
“An influenza pandemic occurs when a new influenza virus appears against which the human population has no immunity, resulting in several simultaneous epidemics worldwide with enormous numbers of deaths and illness.”
This definition was altered in 2009 by WHO to:
“An influenza pandemic may occur when a new influenza virus appears against which the human population has no immunity.”
The current COVID-19 crisis does meet the first criterion of the 2009 onwards WHO definition of a pandemic i.e there is a consensus [see later posts on disputes about this] that SARS CoV2 is a new (corona) virus. However, as immunity to any given disease is in reality a complex and variable phenomenon and I can't see how a total lack the immunity of the "human population" could ever be proven, meeting the second criterion of the WHO definition can never be determined in practise.
Taking the earlier WHO definition and generic dictionary definition of a pandemic in addition to having to be novel and for no prior human immunity to exist, to be considered a pandemic COVID-19 has to affect a "significant proportion" of the population and/or cause "enormous deaths and illness" - to what extent is this true?
If we ignore for the moment concerns over the reliability of COVID-19 deaths statistics from Our World in Data site the numbers of people who died in UK during 2020 were :
All causes: 604,045
Confirmed COVID-19 73,622
So, from a UK population of 66.65 million 73,622 deaths represent just over 1 in 900 people with COVID deaths accounting for about 12% of the deaths on 2020.
Looking at worldwide statistics:
All causes 58.32 Million
COVID-19 1.88 Million
From a world population of 7.674 billion the 1.88 million attributed to COVID-19 represents 0.02% or about 1 in 4000 people and about 3% of all deaths in 2020. Before considering these numbers, one must also consider to what extent COVID-19 affects the "human population” i.e affects everyone equally.
It was established early on in 2020 from Italy that the distribution of COVID-19 deaths was massively unequal. The vast majority of deaths being in the elderly and those with one or more existing serious conditions (comorbidities). According to the ONS for England and Wales the average age of people dying from COVID-19 was 80.3 years whereas the average of people dying from all causes was actually two years younger i.e 78.2 years. The number of people under 24 who died in 2020 whose death involved i.e some may not have been caused by, COVID was some 55 out of a total of 4579 deaths whereas the number of 65 year olds and over whose deaths involved COVID was 77,987 which is 1400 times greater.
From the above :
It is arguable whether COVID-19 is truly a pandemic in the sense of the term generally understood and the definition by the WHO, prior to 2009
Given that most people know less than 900 people it is actually unlikely that the average individual in the UK - a country with one of the highest level of infections and deaths due to COVID-19 - will personally know someone who has died from COVID-19. If they do it is highly likely that person will have been “elderly” and /or with other comorbidities
Given the above some have concluded, perhaps not that unreasonably, that as they and possibly many of their friends' and family don't know anyone who has died of COVID this is somehow all a “scam” or fake issue - this is not a valid conclusion to draw. Despite the true impact of COVID-19 being deliberately exaggerated and serious questions about the accuracy of the official statistics regarding deaths attributed to COVID (see post on PCR tests) excess mortality statistics confirm that many hundreds of thousands of people around the world have died due to some new cause and SARS COV2 is the only credible cause I am aware of. Attempting to claim therefore this is all "fake", a "scamdemic" is simply not true.
European published excess mortality clearly show the impact across Europe of the “first wave” of SARS COV2. The first wave was largely over by week 20 of 2020 yet resulted in an increase in excess mortality across Europe relative to 2018 of some 50 thousand deaths.
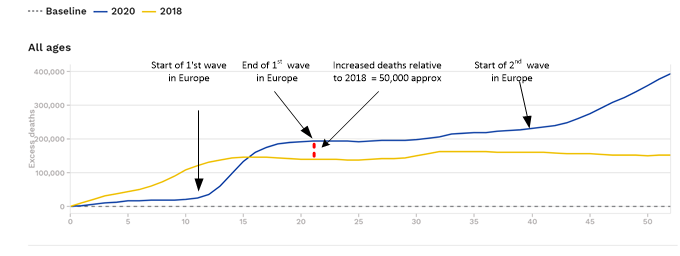
Source https://www.euromomo.eu/graphs-and-maps
I must be noted that, particularly for the second wave, it is impossible to accurately determine from excess mortality statistics alone how much of the increase was caused directly by COVID-19 and how much was due to other factors e.g the policies implemented in early 2020 to deal with it e.g massive cancellation of operations, vastly reduced GP and A&E services, curtailment of screening for diseases like cancer, shortages of medical staff due to enforced isolation, reluctance to visit hospitals and GPs due to fear of infection. Even some mainstream news outlets (but of course not the BBC) reported on a UK ONS public health modelling study carried out in 2020 where the percentage of excess mortality due to the lockdown policies themselves rather than the virus could be as high as 40%.
Even assuming 40% of excess deaths resulted from government policies rather than the virus by the end of 2020 COVID-19 would have been the cause of 150,000 excess deaths across Europe relative to 2018. [i.e 60% of the 250,000 difference at week 52 - see graph above]
The use of the terms pandemic and scamdemic are both to some extent flawed and to differing extents misleading characterizations of the true situation and continue to have serious consequences. Future posts will take a critical look at the consequences of these flawed characterisations.
Notes / References
Groupthink https://www.britannica.com/science/groupthink
Our World in Data Example Plot
Do nothing - 81% of people would be infected 510,000 would die from COVID-19 by August.
Mitigation - 250,000 deaths and completely overwhelm intensive care in the NHS.
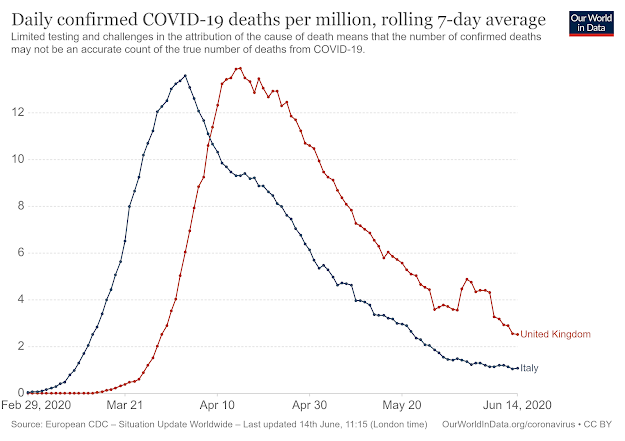 |
| COVID-19 Reported Deaths per Million - UK vs. Italy |
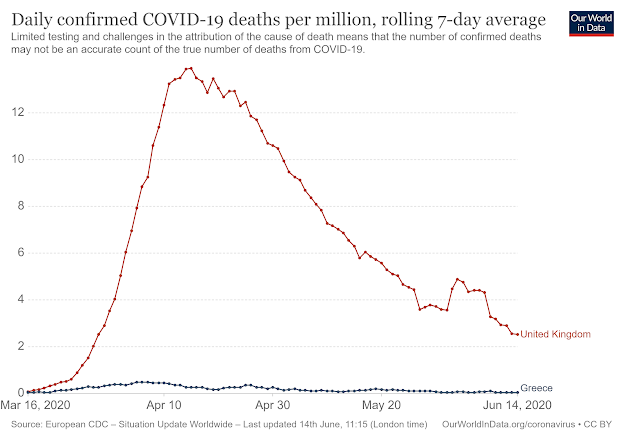 |
| COVID-19 Reported Deaths per Million - UK vs. Greece |
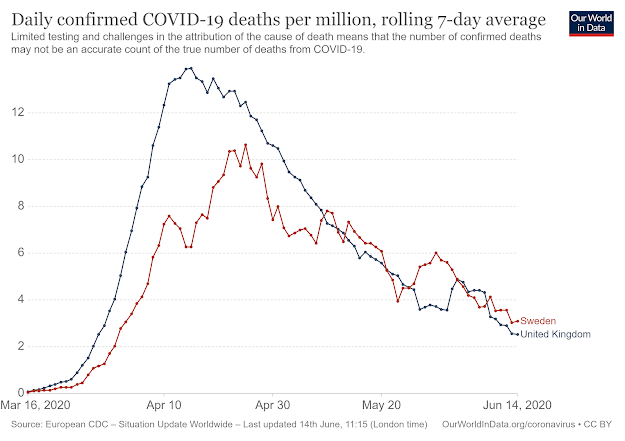 |
| COVID-19 Reported Deaths per Million - UK vs. Sweden |
 |
| COVID-19 Reported Deaths per Million - UK vs. Belarus |
| Projected Deaths - note 1 | Sweden | Belarus | UK |
| Do Nothing | n/a | 69,690 | 500,000 |
| Mitigation only -note 2 | 37,000 | n/a | 250,000 |
| Suppression (lock down) | n/a | n/a | 20,000 - note 3 |
| Total reported to date | 5,053 | 331 | 42,000 |
This set of three posts aim to give a different and more balanced perspective to that being presented in the mainstream media on the current crisis resulting from the the emergence of the new virus, SARS-CoV-2 and the new disease it causes, COVID-19. At the time of writing, June 2020, there are still major gaps in our understanding of how the virus spreads - how many people have been infected by it and how many have died from COVID-19. The various policies implemented by Governments around the world to deal with the impact of this new virus were and continue to be made in a fog of uncertainty and confusion resulting in some very poor decision making that has and will continue to have grave and lasting consequences for huge numbers of people.
 |
| Excess Mortality - 2016 to June 2020 |
 |
| Annual Cumulative Excess Mortality 2018,2019,2020 |
EM (all ages) = 194,284
Total Population = 435,010,967
Age 0 to 14 = 0.00001% or 1 in 7,131,327
Age 15 to 64 = 0.00399% or 1 in 25,063
Over 65 = 0.04046% or 1 in 2,472
The cumulative EM graph for the twenty EU countries shows clearly the higher number of excess deaths in 2020 than in 2018 and 2019. So again, making for now the (false) assumption that all 2020 excess mortality is due solely to COVID-19 then in percentage terms the increase in EM across the 20 countries that can be attributed to COVID-19 is at most.
85% above 2018 and 239% above 2019
“According to new estimates published today, between 291,000 and 646,000 people worldwide die from seasonal influenza-related respiratory illnesses each year, higher than a previous estimate of 250,000 to 500,000 and based on a robust, multinational survey.”https://www.cdc.gov/media/releases/2017/p1213-flu-death-estimate.html
"Risk thresholds for alcohol consumption: combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies"but that's nowhere near as ALARMIST headline grabbing ...


Two legs good - Four legs bad The title of the UK Government policy brought in to attempt to deal with the spread of COVID-19 was “Staying ...
